Patient Education
Conditions We Treat
Back Pain
- Back pain effects more than 85% of all Americans during their lifetime. It can have many causes such as disc pathology, joint pathology, ligament/bone pathology and muscular origins. Pain is usually self-limited and with time should resolve in less than six weeks although if loss of strength, sensory or change in bowel/bladder function occur, this is more urgent and warrants immediate medical attention. Bed rest is not advised nor is the use of lumbar support for more than two weeks. Most sources of pain respond to conservative treatment such a physical therapy, anti-inflamatory medications and topical pair relievers. Acute pain is generally viewed as less than six weeks while chronic pain is generally termed after six months. There is no blood test for pain. The diagnosis and treatment require careful history and physical exam along with proper use of radiographs (xray, CT, MRI) and nerve conduction studies (EMG/NCV) While some back pain presents abruptly after an accident or event (lifting a heavy object) a greater proportion of low back pain occurs insidiously (reaching for a tooth brush). Tumors benign and malignant make up a very small fraction (less than 1%) but need to be considered when neurological symptoms appear and resolution does not occur.
- List of common causes: include muscle strain, degenerative disc disease, disc bulging, disc herniation, joint inflammation (facet and sacroiliac), sciatica (pinched nerve), fractures of vertebrae and lumbar spinal stenosis, prior surgery (post laminectomy syndrome)
- Treatments: For these groups of patients, many will respond to interventional pain procedures, depending on the source of the discomfort. These pain generators and their treatments may include: epidurals, facet blocks
Neck Pain
- This type of pain may not just be limited to the neck but can extend to the head, shoulder and arms. The neck, like the lower back, is composed of many parts, including joints, discs, muscles and nerves. Any of these components can lead to inflammation and pain. For acute pain (less than six weeks onset), most sources of pain respond to conservative treatments, such as physical therapy, chiropractic therapy, anti-inflammatory drugs, oral steroids and possible superficial cortisone injections.
- Unfortunately, there is a subset of people whose pain is so severe that activities or work are extremely limited. Or, the pain extends beyond six weeks. For these groups of patients, many will respond to interventional pain procedures, depending on the source of the discomfort.
- List of common causes: spinal stenosis, herniated disc, degenerative disc, muscle spasms, occipital neuralgia, facet joint disease, atlantoaxial joint disease, cervicogenic headaches
- Treatments: Treatments are determined by the specific cause, which we determine at consult. epidurals, facets
Sciatica
- Can be referred to as as pinched nerve, radiating leg pain, electric shocks, walking pain, standing pain, bending over pain
- List of common causes: can include disc bulge, ruptured disc, pinched nerve, disc herniation, slipped disc
- Treatments are determined by the specific cause, which we determine at consult
- Treatments: epidurals, facets, patients whose pain is resistant to conservative treatment may respond to advanced pain management injections treatments such as transforaminal epidural steroid injections and neuroplasty (lysis of adhesions)
Degenerative Spine
- Associated with spinal bone spurs, degenerative disc disease, spinal stenosis, facet arthritis, arthritic spine, walking pain, standing pain
- List of common causes: This condition is found in most people as they age. For many, this doesn’t cause any pain. For some this can lead to considerable discomfort. This condition be genetic, or as a result of certain life styles or careers.
- Treatments: An MRI may demonstrate the presence of spinal bone spurs. Patients whose pain is resistant to conservative treatment may respond to advanced pain management injections. Several injections are available and specific to the type of pain the patient presents with. These may include but are not limited to transforaminal epidural steroid injections, facet blocks, rhizotomies, epidurals and europlasty.
Spinal Stenosis
- This condition generally occurs over time and leads to narrowing of bone around the spinal cord or spinal nerve roots. The pain that results from lumbar spinal stenosis may include lower back and leg pain. For the cervical region, the pain may involve both the neck and arm.
A subcategory of spinal stenosis includes neurogenic claudication. This condition leads to pain with walking or standing for more than 10 minutes. Frequently, patients must sit for a period of time before the pain will resolve. Characteristically, walking in a shopping mall requires frequent breaks of sitting. - Treatments: With the combination of conservative treatments and epidural steroid injections, many patients will have the pain well controlled. For those that continue to have considerable limitations to walking and standing, options may include spinal surgery or the nonsurgical route of the MILD procedure (minimally invasive lumbar decompression)
RSD/CRPS
- Known as complex regional pain syndrome, reflex sympathetic dystrophy, sympathetic pain. Usually involves arms, hands, legs, feet PAIN
- Telltale signs frequently include: sensitivity to touch, swelling, color changes, temperature changes
- Treatments: Successful treatment of this condition is dependent on early recognition and early intervention. Workup is essential and may include but are not limited radiologic studies, and nerve studies.
- Treatments may include therapy and medications. If ongoing pain continues, therapy is not tolerated, or decreasing function of the effected body part is noted, the patient would then be considered for therapeutic sympathetic nerve blocks. Such examples include a stellate ganglion block or lumbar sympathetic block, performed under fluoroscopic guidance. These injections allow treatment of the pain, increased tolerance to physical therapy, and increased function. The use of IV sedation or monitored anesthesia care is frequently during these procedures used to avoid any discomfort from the procedure itself.
Facet Pain
- This type of pain originates at the facet joint. In the cervical spine, one can experience neck pain with or without shoulder pain, upper arm pain, headaches and facial pain. This type of discomfort can be brought on with changes of neck position and may disrupt one’s sleep.
In the lower back, one can experience pain in multiple areas, including the lower back, buttock, and upper legs. This type of pain is frequently brought on with getting out of bed, getting up from chair, leaning over, or with standing. - Treatments: Radiologic findings may or may not show obvious changes at the facet joint. When conservative treatments, such as therapy and anti-inflammatory drugs fail to provide relief, fluoroscopic directed injections may provide considerable and long term relief. These injections may include diagnostic testing such as facet medial branch nerve blocks and more long term approaches via a rhizotomy.
Sacral Pain / Sacroiliac Joint Inflammation
- Can relate to sacroiliac joint inflammation, tailbone pain, sacral fracture
- This type of pain can be more commonly associated with sitting pain, lying down pain, or experienced with crossing the legs
- Treatments: When conservative treatments, such as therapy and anti-inflammatory drugs fail to provide relief, fluoroscopic directed injections may provide considerable and long term relief.
Occipital Neuralgia
- The occipital pain is routinely experienced at the base of the skull, It can radiate to the top of the head. In fact, occipital neuralgia can mimic other types of headaches. This problem, may be associated with cervicogenic headaches, and degenerative cervical spine.
- Treatments: Coanalgesic medications may help, such as antiseizure medications, antidepressants, muscle relaxants as well as physical therapy.
When this condition persists, the patient may then respond to focus directed injections such as occipital nerve blocks or C2 nerve blocks,
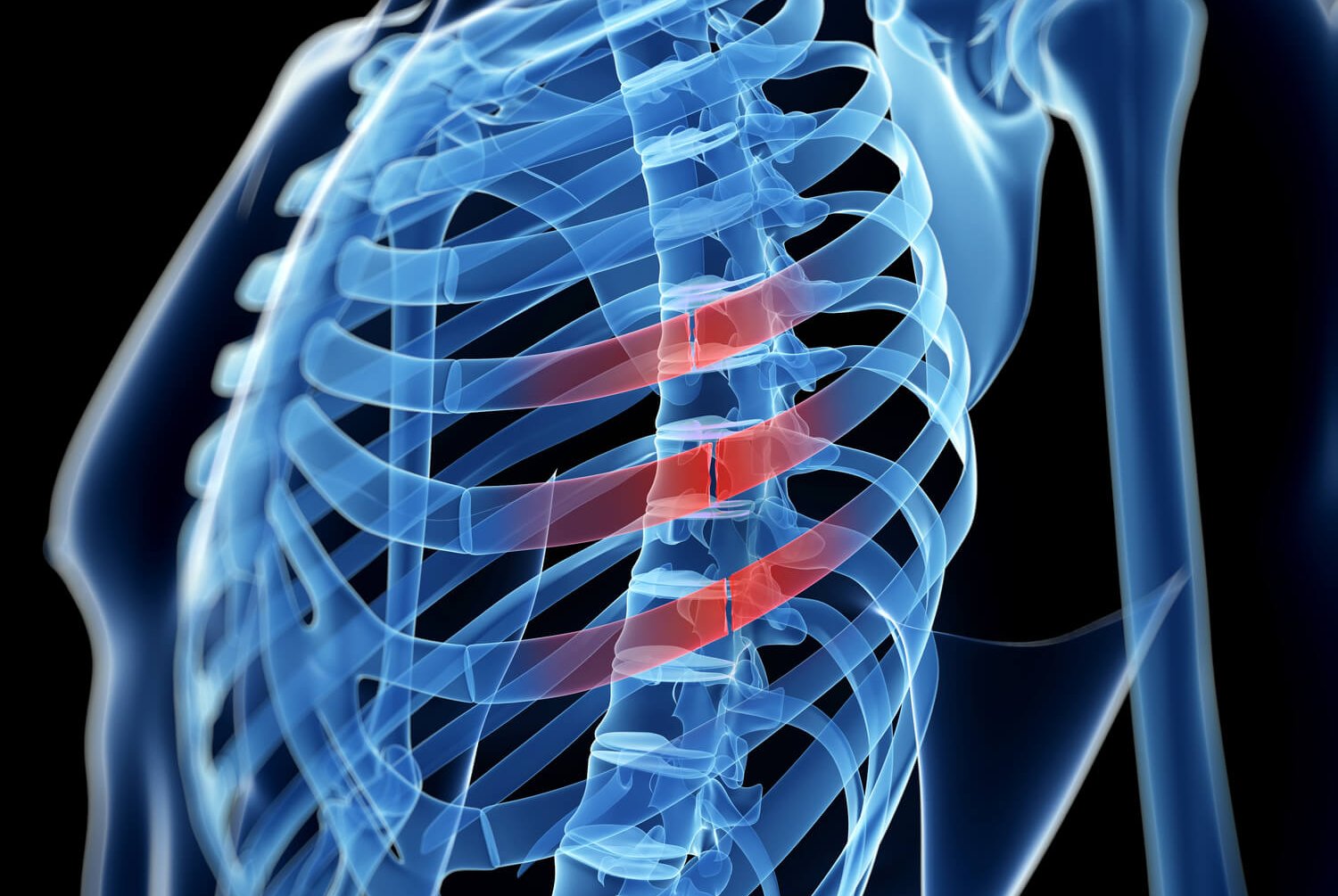
Thoracic Spine Pain
- Also referred to as midback pain, upper back pain. This condition may or may not be accompanied by pain spreading to the sides or chest.
- Common causes may include: degenerative disc disease , thoracic disc herniation, facet joint or vertebral fracture, spinal lesion and spinal stenosis. A comprehensive work up should be included for this type of pain and may include radiologic studies.
- Treatments: Based upon the specific cause, treatments may include conservative approaches, spinal injections, kyphoplasty, and possible surgery.

Knee Pain
- For those patients already diagnosed with arthritis of the knee or with ongoing knee pain despite having knee surgery, multiple treatment options have likely already been considered. These treatments may have included therapy, anti-inflammatory agents, cortisone injections, viscosupplementation injections and consideration of a knee replacement.
- Treatments: For patients that have failed conservative treatment, are reluctant to undergo surgery, are at high risk for surgery or already failed surgery, they may be a candidate for genicular nerve block and subsequent neurotomy/COOLIEF nerve lesioning.
WHIPLASH
- With this condition, one can experience neck pain with or without shoulder pain, upper arm pain, headaches or facial pain. This type of discomfort can be brought on with changes of neck position and may disrupt one’s sleep.
Radiologic findings may or may not show obvious changes at the facet joint - Treatments: When conservative treatments, such as therapy and anti-inflammatory drugs fail to provide relief, fluoroscopic directed injections may provide considerable and long term relief. Such injections may include facet medial branch nerve blocks and more long term treatments via a rhizotomy.
Groin Pain
- Can include hip pain or lower belly pain
- Possible causes include: Post hernia repair, hip arthritis
- Treatments: COOLIEF
Back Pain Even After Having Back Surgery
- This condition may or may not include buttock or leg pain
Sources of this pain may include, spinal stenosis at other levels, facet arthritis, sacroiliac joint inflammation or even scar tissue. Conservative treatments may frequently be dictated by your spine surgeon. If pain persists beyond reasonable expectations, an MRI post surgery will likely be required. - Treatments: Specialized treatments are available for this condition including selective nerve blocks, epidural neuroplasty and even consideration of a spinal cord stimulator trial.
Facial Pain
- Ongoing pain in the face can be due to numerous conditions. Some of these causes include trigeminal neuralgia, supraorbital neuralgia, infraorbital neuralgia, and temporomandibular joint dysfunction (TMJ). For most people suffering from chronic facial pain, multiple medical specialists have already been consulted.
- Treatments: For those people that continue to suffer from considerable pain despite proper treatment, specialized nerve blocks under fluoroscopic guidance may be considered, based upon the diagnosis made.
Shingles / Post Herpetic Neuralgia
- This condition occurs following a painful Shingles outbreak. This type of exquisite pain can be constant, sensitive to touch and travels along the site of the healing rash.
- Common locations of this type of pain include the thoracic spine, chest wall, and near the eye and scalp.
Initial treatments should include an antiviral medication. Other agents may include topical agents, oral neuropathic medications and possibly analgesics. With the persistence of severe pain, this condition than moves into the chronic stage, known as Post Herpetic Neuralgia. - Treatments: Interventional pain treatments, when performed in these early stages, may break the pain cycle and assist with resolution of the pain syndrome.
These include specialized injections called sympathetic blocks, and possibly epidural placed injections.
Other Conditions
- Hip pain, wrist pain, trigeminal neuralgia
Center for Spinal Stenosis
The physicians of Pain Management elected to design and structure the Center for Spinal Stenosis to offer information and the most up-to-date cutting-edge technology to help with the diagnosis and treatment of spinal stenosis.
Learn More
Center for Medical Marijuana
The advantage of using medical marijuana over narcotics is providing pain relief while AVOIDING the unpleasant side effects of constipation, nausea, and respiratory depression. You are unlikely to experience any “high” from the use of medical marijuana.
Learn More